Fundamentals of Pharmaceutical and Biologics Regulations: A Global Perspective
Second Edition
4 Regulatory Affairs Professionals Society
non–small cell lung cancer (NSCLC) under the brand name Iressa
(AstraZeneca) in the US on 13 July 2015. As of March 2025, it is
approved as the generic medicine gefitinib tablets manufactured by
six manufacturers in the US. In the EU, Gefitinib Mylan tablets were
approved in 2018 and withdrawn in 2024 for commercial reasons.
In the EU, a therapeutic biosimilar is not regarded as a ge-
neric medicine of a biological medicine. It is defined as a biologi-
cal medicine highly similar to the reference product, an already
approved biological medicine, in terms of structure, biological ac-
tivity and efficacy, safety, and immunogenicity profile.8 In the US,
a biosimilar is also defined as a biological product that is highly
similar to and has no clinically meaningful differences from an ex-
isting Food and Drug Administration (FDA)–approved reference
product. Minor differences between the biosimilar product and
the reference product in clinically inactive components are ac-
ceptable and must demonstrate no clinically meaningful differ-
ences from the reference product in terms of safety, purity, and
potency (safety and effectiveness).9
Europe has led the way in biosimilar authorizations. In April
2006, Sandoz received marketing authorization (MA) for Om-
nitrope (somatropin),10 a biosimilar to Pfizer’s Genotropin (so-
matropin), from the European Commission (EC), becoming the
world’s first biosimilar. Japan and Canada followed with authori-
zations in 2009. On 6 March 2015, Sandoz received authorization
for the first US biosimilar, Zarxio (filgrastim-sndz), a biosimilar to
Amgen’s Neupogen (filgrastim).11
These above approaches leverage the information previously
submitted for pharmacology, formulation, safety (toxicology), and
previous human experience, thereby reducing development time,
cost, and resources and reducing the risk of product failures in
clinical development. The two approaches do not require the com-
pany to repeat nonclinical (Step 2) research. Instead, a biosimilar
usually requires an abbreviated nonclinical program only. For a ge-
neric approach, clinical research (Step 3) is not repeated on inac-
tive ingredients or formulations already authorized for safety and
effectiveness. The generic medicine must be bioequivalent to the
innovator reference product. For a biosimilar approach, new clini-
cal trials to demonstrate similarity to the reference medicine are
conducted to determine human pharmacokinetics (exposure) and
pharmacodynamics (response), and clinical immunogenicity. In
addition, a regulatory agency may require a new abbreviated clinical
trial for safety and effectiveness for the biosimilar to be authorized.
Another effective alternative approach to traditional drug de-
velopment is drug repurposing (DR). These medicines generally
share a similar active substance with an already authorized product
but may differ significantly in their formulation, strength, route of
administration, or indications. Such differences introduce addi-
tional value, enhancing therapeutic outcomes or addressing patient
needs that existing generics may not fully meet.
DR identifies new uses for existing drugs and finds new ther-
apeutic uses for new drugs other than the disease for which they
were initially intended. DR is also known as repositioning, recy-
cling, rescuing, and reprofiling.
Two well-known success stories of DR are sildenafil, mar-
keted as Viagra, and thalidomide. Viagra represents unintended or
accidental repurposing. During a clinical trial for a potential new
drug to treat angina, Pfizer observed that many male participants
reported unusual side effects, erections.12 Before Viagra was ap-
proved in 1998, there was no oral treatment for erectile dysfunc-
tion. Originally developed as an anti-hypertensive, sildenafil has
been repurposed to treat erectile dysfunction and pulmonary arte-
rial hypertension. Thalidomide, a widely used drug in Europe in
the 1950s and 1960s for the treatment of nausea in pregnant
women, was connected to serious birth defects (fetal limb) and re-
moved from the market in 1961.13 Recently, research has shown it
to be an effective treatment for leprosy and multiple myeloma.14
A more recent example of DR – more specifically, reposition-
ing – is Keytruda (pembrolizumab), an anti–PD-1 antibody origi-
nally approved in 2014 to treat advanced or unresectable
melanoma. Keytruda subsequently has been approved for addi-
tional indications, in combination with approved therapies/treat-
ments, and for use in different treatment settings.15 As of this
writing, Keytruda was indicated to treat 20 different cancers.
While the de novo development process has five steps, the
DR process has four steps: compound selection and validation,
clinical development, regulatory authority review and authoriza-
tion, and market access, including postmarketing safety monitor-
ing and reporting.15
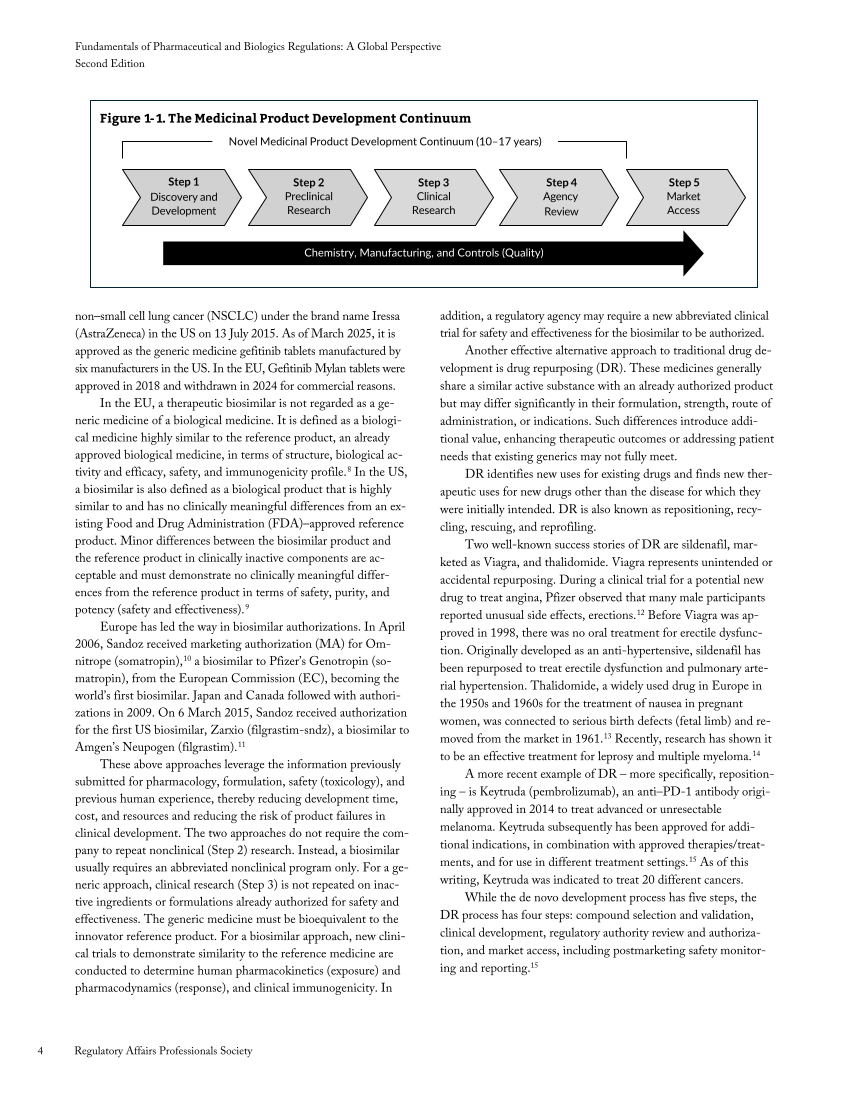
Novel Medicinal Product Development Continuum (10–17 years)
Step 1
Discovery and
Development
Step 2
Preclinical
Research
Step 3
Clinical
Research
Step 4
Agency
Review
Step 5
Market
Access
Chemistry, Manufacturing, and Controls (Quality)
Figure 1-1. The Medicinal Product Development Continuum
Second Edition
4 Regulatory Affairs Professionals Society
non–small cell lung cancer (NSCLC) under the brand name Iressa
(AstraZeneca) in the US on 13 July 2015. As of March 2025, it is
approved as the generic medicine gefitinib tablets manufactured by
six manufacturers in the US. In the EU, Gefitinib Mylan tablets were
approved in 2018 and withdrawn in 2024 for commercial reasons.
In the EU, a therapeutic biosimilar is not regarded as a ge-
neric medicine of a biological medicine. It is defined as a biologi-
cal medicine highly similar to the reference product, an already
approved biological medicine, in terms of structure, biological ac-
tivity and efficacy, safety, and immunogenicity profile.8 In the US,
a biosimilar is also defined as a biological product that is highly
similar to and has no clinically meaningful differences from an ex-
isting Food and Drug Administration (FDA)–approved reference
product. Minor differences between the biosimilar product and
the reference product in clinically inactive components are ac-
ceptable and must demonstrate no clinically meaningful differ-
ences from the reference product in terms of safety, purity, and
potency (safety and effectiveness).9
Europe has led the way in biosimilar authorizations. In April
2006, Sandoz received marketing authorization (MA) for Om-
nitrope (somatropin),10 a biosimilar to Pfizer’s Genotropin (so-
matropin), from the European Commission (EC), becoming the
world’s first biosimilar. Japan and Canada followed with authori-
zations in 2009. On 6 March 2015, Sandoz received authorization
for the first US biosimilar, Zarxio (filgrastim-sndz), a biosimilar to
Amgen’s Neupogen (filgrastim).11
These above approaches leverage the information previously
submitted for pharmacology, formulation, safety (toxicology), and
previous human experience, thereby reducing development time,
cost, and resources and reducing the risk of product failures in
clinical development. The two approaches do not require the com-
pany to repeat nonclinical (Step 2) research. Instead, a biosimilar
usually requires an abbreviated nonclinical program only. For a ge-
neric approach, clinical research (Step 3) is not repeated on inac-
tive ingredients or formulations already authorized for safety and
effectiveness. The generic medicine must be bioequivalent to the
innovator reference product. For a biosimilar approach, new clini-
cal trials to demonstrate similarity to the reference medicine are
conducted to determine human pharmacokinetics (exposure) and
pharmacodynamics (response), and clinical immunogenicity. In
addition, a regulatory agency may require a new abbreviated clinical
trial for safety and effectiveness for the biosimilar to be authorized.
Another effective alternative approach to traditional drug de-
velopment is drug repurposing (DR). These medicines generally
share a similar active substance with an already authorized product
but may differ significantly in their formulation, strength, route of
administration, or indications. Such differences introduce addi-
tional value, enhancing therapeutic outcomes or addressing patient
needs that existing generics may not fully meet.
DR identifies new uses for existing drugs and finds new ther-
apeutic uses for new drugs other than the disease for which they
were initially intended. DR is also known as repositioning, recy-
cling, rescuing, and reprofiling.
Two well-known success stories of DR are sildenafil, mar-
keted as Viagra, and thalidomide. Viagra represents unintended or
accidental repurposing. During a clinical trial for a potential new
drug to treat angina, Pfizer observed that many male participants
reported unusual side effects, erections.12 Before Viagra was ap-
proved in 1998, there was no oral treatment for erectile dysfunc-
tion. Originally developed as an anti-hypertensive, sildenafil has
been repurposed to treat erectile dysfunction and pulmonary arte-
rial hypertension. Thalidomide, a widely used drug in Europe in
the 1950s and 1960s for the treatment of nausea in pregnant
women, was connected to serious birth defects (fetal limb) and re-
moved from the market in 1961.13 Recently, research has shown it
to be an effective treatment for leprosy and multiple myeloma.14
A more recent example of DR – more specifically, reposition-
ing – is Keytruda (pembrolizumab), an anti–PD-1 antibody origi-
nally approved in 2014 to treat advanced or unresectable
melanoma. Keytruda subsequently has been approved for addi-
tional indications, in combination with approved therapies/treat-
ments, and for use in different treatment settings.15 As of this
writing, Keytruda was indicated to treat 20 different cancers.
While the de novo development process has five steps, the
DR process has four steps: compound selection and validation,
clinical development, regulatory authority review and authoriza-
tion, and market access, including postmarketing safety monitor-
ing and reporting.15
Novel Medicinal Product Development Continuum (10–17 years)
Step 1
Discovery and
Development
Step 2
Preclinical
Research
Step 3
Clinical
Research
Step 4
Agency
Review
Step 5
Market
Access
Chemistry, Manufacturing, and Controls (Quality)
Figure 1-1. The Medicinal Product Development Continuum