Fundamentals of Pharmaceutical and Biologics Regulations: A Global Perspective
Second Edition
14 Regulatory Affairs Professionals Society
price. Prescribers and patients need immediate, consistent, and con-
tinued access to medicines once approved and available.
Often, market access and activities are planned closer to mar-
keting application, submission, authorization, and launch. To be
successful, however, market access planning should be part of the
process from early development through post-launch. That plan-
ning should provide input into the target product profile and other
key development input, such as patient preferences, quality-of-life
metrics, health behaviors, symptoms, and health status.
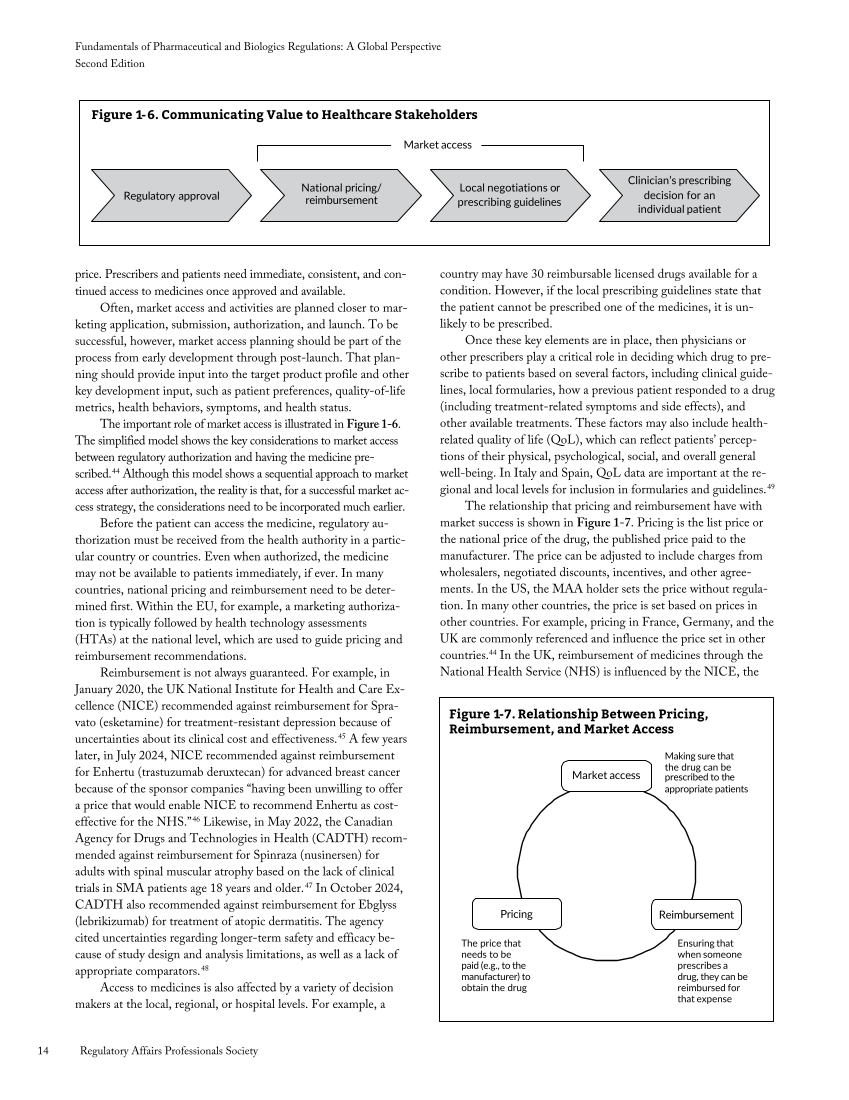
The important role of market access is illustrated in Figure 1-6.
The simplified model shows the key considerations to market access
between regulatory authorization and having the medicine pre-
scribed.44 Although this model shows a sequential approach to market
access after authorization, the reality is that, for a successful market ac-
cess strategy, the considerations need to be incorporated much earlier.
Before the patient can access the medicine, regulatory au-
thorization must be received from the health authority in a partic-
ular country or countries. Even when authorized, the medicine
may not be available to patients immediately, if ever. In many
countries, national pricing and reimbursement need to be deter-
mined first. Within the EU, for example, a marketing authoriza-
tion is typically followed by health technology assessments
(HTAs) at the national level, which are used to guide pricing and
reimbursement recommendations.
Reimbursement is not always guaranteed. For example, in
January 2020, the UK National Institute for Health and Care Ex-
cellence (NICE) recommended against reimbursement for Spra-
vato (esketamine) for treatment-resistant depression because of
uncertainties about its clinical cost and effectiveness.45 A few years
later, in July 2024, NICE recommended against reimbursement
for Enhertu (trastuzumab deruxtecan) for advanced breast cancer
because of the sponsor companies “having been unwilling to offer
a price that would enable NICE to recommend Enhertu as cost-
effective for the NHS.”46 Likewise, in May 2022, the Canadian
Agency for Drugs and Technologies in Health (CADTH) recom-
mended against reimbursement for Spinraza (nusinersen) for
adults with spinal muscular atrophy based on the lack of clinical
trials in SMA patients age 18 years and older.47 In October 2024,
CADTH also recommended against reimbursement for Ebglyss
(lebrikizumab) for treatment of atopic dermatitis. The agency
cited uncertainties regarding longer-term safety and efficacy be-
cause of study design and analysis limitations, as well as a lack of
appropriate comparators.48
Access to medicines is also affected by a variety of decision
makers at the local, regional, or hospital levels. For example, a
country may have 30 reimbursable licensed drugs available for a
condition. However, if the local prescribing guidelines state that
the patient cannot be prescribed one of the medicines, it is un-
likely to be prescribed.
Once these key elements are in place, then physicians or
other prescribers play a critical role in deciding which drug to pre-
scribe to patients based on several factors, including clinical guide-
lines, local formularies, how a previous patient responded to a drug
(including treatment-related symptoms and side effects), and
other available treatments. These factors may also include health-
related quality of life (QoL), which can reflect patients’ percep-
tions of their physical, psychological, social, and overall general
well-being. In Italy and Spain, QoL data are important at the re-
gional and local levels for inclusion in formularies and guidelines.49
The relationship that pricing and reimbursement have with
market success is shown in Figure 1-7. Pricing is the list price or
the national price of the drug, the published price paid to the
manufacturer. The price can be adjusted to include charges from
wholesalers, negotiated discounts, incentives, and other agree-
ments. In the US, the MAA holder sets the price without regula-
tion. In many other countries, the price is set based on prices in
other countries. For example, pricing in France, Germany, and the
UK are commonly referenced and influence the price set in other
countries.44 In the UK, reimbursement of medicines through the
National Health Service (NHS) is influenced by the NICE, the
Market access
Regulatory approval
National pricing/
reimbursement
Local negotiations or
prescribing guidelines
Clinician’s prescribing
decision for an
individual patient
Figure 1-6. Communicating Value to Healthcare Stakeholders
Making sure that
the drug can be
Market access prescribed to the
appropriate patients
Pricing Reimbursement
The price that
needs to be
paid (e.g., to the
manufacturer) to
obtain the drug
Ensuring that
when someone
prescribes a
drug, they can be
reimbursed for
that expense
Figure 1-7. Relationship Between Pricing,
Reimbursement, and Market Access
Second Edition
14 Regulatory Affairs Professionals Society
price. Prescribers and patients need immediate, consistent, and con-
tinued access to medicines once approved and available.
Often, market access and activities are planned closer to mar-
keting application, submission, authorization, and launch. To be
successful, however, market access planning should be part of the
process from early development through post-launch. That plan-
ning should provide input into the target product profile and other
key development input, such as patient preferences, quality-of-life
metrics, health behaviors, symptoms, and health status.
The important role of market access is illustrated in Figure 1-6.
The simplified model shows the key considerations to market access
between regulatory authorization and having the medicine pre-
scribed.44 Although this model shows a sequential approach to market
access after authorization, the reality is that, for a successful market ac-
cess strategy, the considerations need to be incorporated much earlier.
Before the patient can access the medicine, regulatory au-
thorization must be received from the health authority in a partic-
ular country or countries. Even when authorized, the medicine
may not be available to patients immediately, if ever. In many
countries, national pricing and reimbursement need to be deter-
mined first. Within the EU, for example, a marketing authoriza-
tion is typically followed by health technology assessments
(HTAs) at the national level, which are used to guide pricing and
reimbursement recommendations.
Reimbursement is not always guaranteed. For example, in
January 2020, the UK National Institute for Health and Care Ex-
cellence (NICE) recommended against reimbursement for Spra-
vato (esketamine) for treatment-resistant depression because of
uncertainties about its clinical cost and effectiveness.45 A few years
later, in July 2024, NICE recommended against reimbursement
for Enhertu (trastuzumab deruxtecan) for advanced breast cancer
because of the sponsor companies “having been unwilling to offer
a price that would enable NICE to recommend Enhertu as cost-
effective for the NHS.”46 Likewise, in May 2022, the Canadian
Agency for Drugs and Technologies in Health (CADTH) recom-
mended against reimbursement for Spinraza (nusinersen) for
adults with spinal muscular atrophy based on the lack of clinical
trials in SMA patients age 18 years and older.47 In October 2024,
CADTH also recommended against reimbursement for Ebglyss
(lebrikizumab) for treatment of atopic dermatitis. The agency
cited uncertainties regarding longer-term safety and efficacy be-
cause of study design and analysis limitations, as well as a lack of
appropriate comparators.48
Access to medicines is also affected by a variety of decision
makers at the local, regional, or hospital levels. For example, a
country may have 30 reimbursable licensed drugs available for a
condition. However, if the local prescribing guidelines state that
the patient cannot be prescribed one of the medicines, it is un-
likely to be prescribed.
Once these key elements are in place, then physicians or
other prescribers play a critical role in deciding which drug to pre-
scribe to patients based on several factors, including clinical guide-
lines, local formularies, how a previous patient responded to a drug
(including treatment-related symptoms and side effects), and
other available treatments. These factors may also include health-
related quality of life (QoL), which can reflect patients’ percep-
tions of their physical, psychological, social, and overall general
well-being. In Italy and Spain, QoL data are important at the re-
gional and local levels for inclusion in formularies and guidelines.49
The relationship that pricing and reimbursement have with
market success is shown in Figure 1-7. Pricing is the list price or
the national price of the drug, the published price paid to the
manufacturer. The price can be adjusted to include charges from
wholesalers, negotiated discounts, incentives, and other agree-
ments. In the US, the MAA holder sets the price without regula-
tion. In many other countries, the price is set based on prices in
other countries. For example, pricing in France, Germany, and the
UK are commonly referenced and influence the price set in other
countries.44 In the UK, reimbursement of medicines through the
National Health Service (NHS) is influenced by the NICE, the
Market access
Regulatory approval
National pricing/
reimbursement
Local negotiations or
prescribing guidelines
Clinician’s prescribing
decision for an
individual patient
Figure 1-6. Communicating Value to Healthcare Stakeholders
Making sure that
the drug can be
Market access prescribed to the
appropriate patients
Pricing Reimbursement
The price that
needs to be
paid (e.g., to the
manufacturer) to
obtain the drug
Ensuring that
when someone
prescribes a
drug, they can be
reimbursed for
that expense
Figure 1-7. Relationship Between Pricing,
Reimbursement, and Market Access